doktorekg.com
Left Posterior Fascicular Block (LPFB) - Left Posterior Hemiblock
Diagnostic criteria
 QRS width is less than 120 ms.
QRS width is less than 120 ms.
The QRS axis at the frontal plane is between 90 degrees and 180 degrees:
right axis deviation.
For isolated LPFB, other causes of right axis deviation:
- vertical heart in a slender person,
- right ventricular hypertrophy,
- large lateral infarction should be absent.
There is rS pattern in leads D1
and aVL.
There is qR pattern in leads D3
and aVF.
Clinical significance
Isolated LPFB is very rare.
LPFB usually accompanies right bundle branch block (RBBB).
The development of RBBB + LPFB during acute myocardial infarction is a sign of poor prognosis.
RBBB + LPFB has a high probability to turn into complete AV block.
References
Circulation 2009;119:e235-e240
Circulation 2007;115:1154-1163

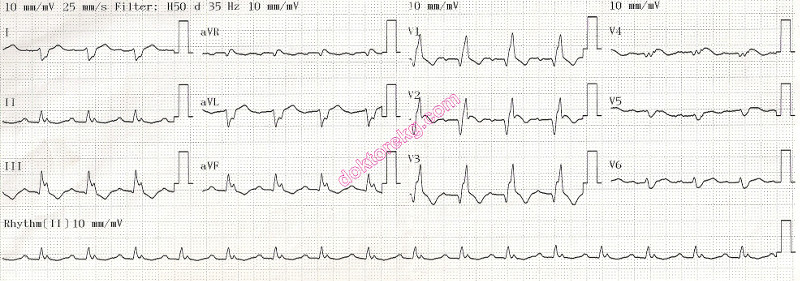
ECG 1. Left posterior fascicular block.
Click here for a more detailed ECG

ECG 2. Left posterior fascicular block in a 39 years-old man.
Click here for a more detailed ECG

ECG 3. Left posterior fascicular block in another patient.
Click here for a more detailed ECG

ECG 4. The above ECG belongs to a 62 year old woman with coronary artery disease, chronic obstructive lung disease and
systemic hypertension. In addition to the left posterior fascicular block, there are also right bundle branch block, right atrial
abnormality and left atrial abnormality.
Click here for a more detailed ECG

ECG 5. The ECG above belongs to a 78 years-old woman who had undergone coronary artery bypass surgery.
LPFB and RBBB are seen.
Click here for a more detailed ECG

ECG 6. The ECG above belongs to a 75 years-old hypertensive woman who had undergone coronary artery bypass surgery
because of 3-vessel disease. LPFB and RBBB are seen.
Click here for a more detailed ECG

ECG 7. The ECG above belongs to a 55 years-old man. LPFB and RBBB are seen.
Click here for a more detailed ECG

ECG 8. The ECG above belongs to a 78 years-old man. LPFB, RBBB and frequent VPCs are seen.
Click here for a more detailed ECG

ECG 9. The ECG above belongs to a 76 years-old woman with obstruction of the right coronary and circumflex arteries.
She has hypertension and left ventricular hypertrophy. Echocardiography showed interventricular septal thickness as 1.7 cm
and posterior wall thickness as 1.2 cm. The ECG shows both LPFB and RBBB.
Click here for a more detailed ECG

ECG 10. The ECG above belongs to a 10 years-old girl with a normal ECHOcardiogram.
Incomplete right bundle branch block (RBBB pattern) is accompanied by left posterior fascicular block.
QRS axis is about + 120 degrees (right axis deviation).
Pediatric cardiologist Dr. Mahmut Gokdemir has donated this ECG to our website.
Click here for a more detailed ECG
ECG 11a. The above ECG is from a 63 years-old man who was admitted lately to the hospital while experiencing acute anterior wall myocardial infarction.
The above ECG was recorded 24 hours after stenting of the LAD coronary artery.
Right bundle branch block and sinus rhythm is seen. Precordial leads show Q waves while lacking ST segment elevation.
1st degree AV block and left posterior fascicular block are also seen.
Click here for a more detailed ECG

ECG 11b. Above is his ECG which was recorded several hours after ECG 11a. It shows atrial tachycardia and complete AV block.
Shape of the P waves in ECG 11b are different than that of the ECG 11a: atrial tachycardia with block.
The wide QRS complexes also have a different configuration than QRS complexes of the RBBB pattern: idioventricular rhythm.
Because of anterior myocardial infarction and late admission to the hospital, the left ventricular systolic function is compromised.
Now, complete AV block interferes with contribution of atrial contractions to the cardiac output.
Ventricular (QRS) rate is low due to idioventricular rhythm.
Therefore, the patient had signs of low cardiac output while the above ECG was recorded.
He received temporary cardiac pacemaker after recording of the above ECG.
Click here for a more detailed ECG
QRS width is less than 120 ms.
The QRS axis at the frontal plane is between 90 degrees and 180 degrees:
right axis deviation.
For isolated LPFB, other causes of right axis deviation:
- vertical heart in a slender person,
- right ventricular hypertrophy,
- large lateral infarction should be absent.
There is rS pattern in leads D1
and aVL.
There is qR pattern in leads D3
and aVF.
Clinical significance
Isolated LPFB is very rare.
LPFB usually accompanies right bundle branch block (RBBB).
The development of RBBB + LPFB during acute myocardial infarction is a sign of poor prognosis.
RBBB + LPFB has a high probability to turn into complete AV block.
References
Circulation 2009;119:e235-e240
Circulation 2007;115:1154-1163
ECG 1. Left posterior fascicular block.
Click here for a more detailed ECG
ECG 2. Left posterior fascicular block in a 39 years-old man.
Click here for a more detailed ECG
ECG 3. Left posterior fascicular block in another patient.
Click here for a more detailed ECG
ECG 4. The above ECG belongs to a 62 year old woman with coronary artery disease, chronic obstructive lung disease and
systemic hypertension. In addition to the left posterior fascicular block, there are also right bundle branch block, right atrial
abnormality and left atrial abnormality.
Click here for a more detailed ECG
ECG 5. The ECG above belongs to a 78 years-old woman who had undergone coronary artery bypass surgery.
LPFB and RBBB are seen.
Click here for a more detailed ECG
ECG 6. The ECG above belongs to a 75 years-old hypertensive woman who had undergone coronary artery bypass surgery
because of 3-vessel disease. LPFB and RBBB are seen.
Click here for a more detailed ECG
ECG 7. The ECG above belongs to a 55 years-old man. LPFB and RBBB are seen.
Click here for a more detailed ECG
ECG 8. The ECG above belongs to a 78 years-old man. LPFB, RBBB and frequent VPCs are seen.
Click here for a more detailed ECG
ECG 9. The ECG above belongs to a 76 years-old woman with obstruction of the right coronary and circumflex arteries.
She has hypertension and left ventricular hypertrophy. Echocardiography showed interventricular septal thickness as 1.7 cm
and posterior wall thickness as 1.2 cm. The ECG shows both LPFB and RBBB.
Click here for a more detailed ECG
ECG 10. The ECG above belongs to a 10 years-old girl with a normal ECHOcardiogram.
Incomplete right bundle branch block (RBBB pattern) is accompanied by left posterior fascicular block.
QRS axis is about + 120 degrees (right axis deviation).
Pediatric cardiologist Dr. Mahmut Gokdemir has donated this ECG to our website.
Click here for a more detailed ECG
ECG 11a. The above ECG is from a 63 years-old man who was admitted lately to the hospital while experiencing acute anterior wall myocardial infarction.
The above ECG was recorded 24 hours after stenting of the LAD coronary artery.
Right bundle branch block and sinus rhythm is seen. Precordial leads show Q waves while lacking ST segment elevation.
1st degree AV block and left posterior fascicular block are also seen.
Click here for a more detailed ECG
ECG 11b. Above is his ECG which was recorded several hours after ECG 11a. It shows atrial tachycardia and complete AV block.
Shape of the P waves in ECG 11b are different than that of the ECG 11a: atrial tachycardia with block.
The wide QRS complexes also have a different configuration than QRS complexes of the RBBB pattern: idioventricular rhythm.
Because of anterior myocardial infarction and late admission to the hospital, the left ventricular systolic function is compromised.
Now, complete AV block interferes with contribution of atrial contractions to the cardiac output.
Ventricular (QRS) rate is low due to idioventricular rhythm.
Therefore, the patient had signs of low cardiac output while the above ECG was recorded.
He received temporary cardiac pacemaker after recording of the above ECG.
Click here for a more detailed ECG