doktorekg.com
Third Degree (Complete) Atrioventricular Block
Last update: May 2020
Diagnostic criteria
 Atria and ventricles depolarize independently:
Atria and ventricles depolarize independently:
- P waves are regular in themselves and QRS waves are regular among themselves.
- Every P wave is not followed by a QRS complex.
- Some QRS complexes may coincidentally have preceeding P waves,
- Some QRS complexes may have P waves buried in them.
- Some P waves, buried in the QRS, will deform the QRS complex and may falsely give the impression of delta wave and therefore intermittent WPW syndrome, at first glance.
If the escape rhythm is junctional, then heart rate is
40-60/minute with narrow QRS complexes.
If the escape rhythm is idioventricular, then heart rate is
20-40/minute with wide QRS complexes.
Equalization of R-R intervals in a patient with atrial fibrillation suggests development of complete AV block.
In patients with atrial fibrillation who are already under Digoxin therapy, equalization of R-R intervals suggests development of complete AV block due to Digoxin intoxication.
Rarely, complete AV block may be congenital.
References (some with links to free full text and sample ECGs)
Surawicz, Knilans. Chou's electrocardiography in clinical practice. 6th edition. Saunders. Philadelphia 2008.
Circulation 1995;92(3):442-449.
Br Med J (Clin Res Ed) 1983;286(6380):1769-1770.
Circulation 1995;92(3):283-285.
Br Heart J 1989;62(4):320-324.
G Ital Cardiol 1993;23(1):39-53.
Br Heart J 1990;64(5):338-339.
Clin Cardiol 1984;7(6):356-362.
Am J Cardiol 1991;67(4):225-230.
J Postgrad Med 1991;37(1):58B, 59-61.
J Clin Invest 1989;84(2):627-634.
Br Heart J 1988;60(6):512-515.

ECG 1. Third degree (complete) AV block in a 68 years-old woman with Systemic Sclerosis (Scleroderma).
Multidetector CT coronary angiography showed normal coronary arteries.
Click here for a more detailed ECG
The ECG above has been used with the permission of Anatolian Journal of Cardiology and AVES Publishing.
Click here to see the related article of Dr. Canpolat et al.

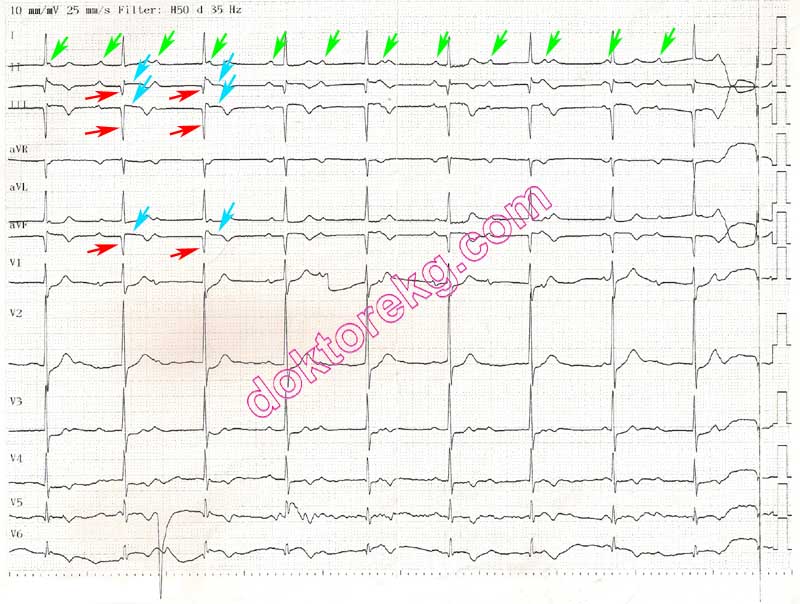
ECG 2. Third degree (complete) AV block. P waves are completely unrelated to the QRS complexes.
Click here for a more detailed ECG

ECG 3. The rhythm strip at the bottom of the above tracing shows complete AV block on the left ( P waves are not related to
QRS complexes ) which is then followed by 2:1 AV block ( only 1 of every two P waves is conducted ).
Click here for a more detailed ECG

ECG 4. The left side of above ECG shows complete AV block. P waves are not related to QRS complexes.
Some P waves, buried in the QRS, deform the QRS complex and give the impression of intermittent WPW syndrome at first glance
The right side shows Wenkebach AV block.
PR interval gradually prolongs; 3rd and 6th P waves are dropped (not conducted to the ventricles).
Click here for a more detailed ECG
ECG 5. The ECG above belongs to a 58 years-old man who admitted lately to the hospital and was diagnosed as
inferior myocardial infarction.
Q waves , ST segment elevation and negative T waves are seen in inferior leads.
Also, the P waves are not related to the QRS complexes : complete AV block .
Click here for a more detailed ECG

ECG 6. The ECG above belongs to a 55 years-old woman who developed persistent av block (A) after consumption of
Grayanotoxin-containing mad honey. The ECG on the right (B) was recorded after implantation of a permanent pacemaker.
Coronary angiography showed normal coronary arteries.
Click here for a more detailed ECG
The ECG above has been used with the permission of Anatolian Journal of Cardiology and AVES Publishing.
Click here to read the relevant article of Dr. Canpolat et al.

ECG 7. Complete AV block during acute myocardial infarction.
P waves are not related to QRS complexes.
Click here for a more detailed ECG

ECG 8. The ECG above shows complete AV block. P waves are not related to the QRS complexes,
At times, P waves are seen in front or at the end of the QRS complexes and distort them.
Pediatric cardiologist Prof. Dr. Birgul Varan has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 9a. The ECG above is from a 6 months-old baby with congenital complete AV block.
P waves are not related to the QRS complexes. Therefore, some P waves are buried in the QRS complexes.
P wave rate is normal for a baby; not to be confused with atrial flutter or atrial tachycardia.
Pediatric cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 9b. Rhythm tracing from the same baby: complete AV block is seen. P waves are not related to the QRS complexes.
P wave rate is normal for a baby; not to be confused with atrial flutter or atrial tachycardia.
Pediatric cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 10a. The above ECG shows both complete AV block and interatrial block. It was recorded during acute inferior wall myocardial infarction. P waves are not related to the QRS complexes. Therefore, some P waves are buried in QRS complexes. The P wave width is slightly more than 120 milliseconds: interatrial block. This ECG was recorded at a calibration of 20 mm/mV to show interatrial block. The P wave morphology and PR interval are also compatible with atrial infarction. Displacement of the PQ interval is considered the most useful sign of atrial infarction. The displacement of PQ interval during atrial infarction is best appreciated in patients with AV block.
Click here for a more detailed ECG

A close-up view of PR segment elevation from the ECG 10a is seen above. This is a magnified view of the P wave before the 8th QRS complex in lead II from the ECG 10a. The PR segment is elevated when compared with the baseline (TP segment).

ECG 10b. Above is his ECG at a standard 10 mm/mV calibration.
It is difficult to see interatrial block, PR segment elevation and complete AV block, at first glance.
Click here for a more detailed ECG

ECG 11a. The ECG above is from a 95 years-old woman with atrial fibrillation and complete av block.
Although atrial fibrillation is known as an "irregularly irregular rhythm", it becomes a regular rhythm
when complete av block developes. RR intervals are regular in the above ECG.
The above ECG is recorded at a standard calibration of 10mm/mV and the fibrillatory waves are hardly noticeable.
Click here for a more detailed ECG
ECG 11b. The above ECG belongs to the same patient.
It is recorded at a calibration of 20 mm/mV.
Now, it is more easy to see the fibrillatory waves.
The RR intervals are equal (regular) due to complete AV block.
Click here for a more detailed ECG
ECG 12a. Above is an ECG from a 44 years-old woman who had undergone catheter ablation of
supraventricular tachycardia 2 weeks ago. Complete AV block has developed during ablation.
Complete AV block is seen in the above ECG. Some QRS complexes are narrow (nodal beats) some are wide (ventricular beats).
The complete AV block is intermittent. To the right of the above ECG, the block disappears and
every P wave is followed by a QRS complex
Click here for a more detailed ECG

ECG 12b. The ECG above belongs to the same patient. It was recorded immediately after the ECG 12a.
Now, there is no complete AV block. The rhythm is sinus with right bundle branch block.
Click here for a more detailed ECG

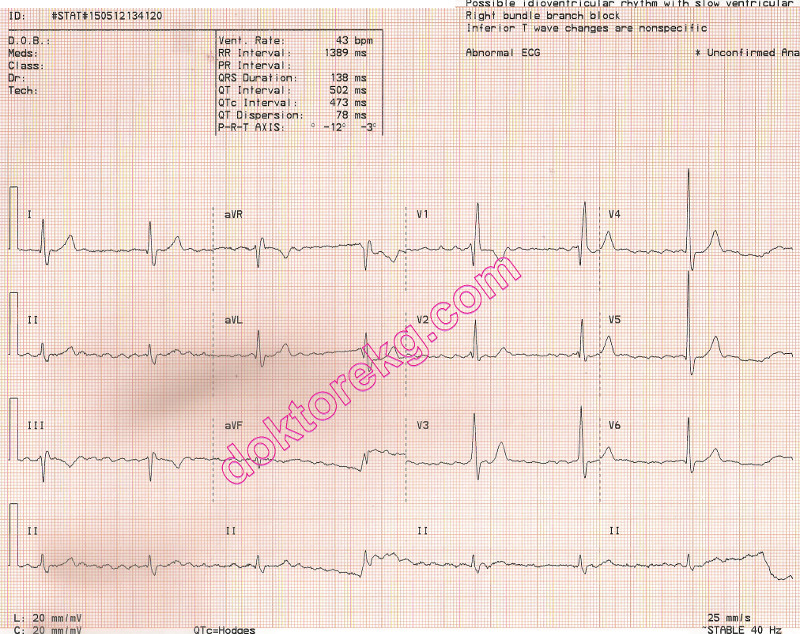
ECG 13. The ECG above shows complete AV block. P waves are not related to the QRS complexes,
There is also right bundle branch block.
It was recorded 5 days after Bentall operation.
Click here for a more detailed ECG
Diagnostic criteria
Atria and ventricles depolarize independently:
- P waves are regular in themselves and QRS waves are regular among themselves.
- Every P wave is not followed by a QRS complex.
- Some QRS complexes may coincidentally have preceeding P waves,
- Some QRS complexes may have P waves buried in them.
- Some P waves, buried in the QRS, will deform the QRS complex and may falsely give the impression of delta wave and therefore intermittent WPW syndrome, at first glance.
If the escape rhythm is junctional, then heart rate is
40-60/minute with narrow QRS complexes.
If the escape rhythm is idioventricular, then heart rate is
20-40/minute with wide QRS complexes.
Equalization of R-R intervals in a patient with atrial fibrillation suggests development of complete AV block.
In patients with atrial fibrillation who are already under Digoxin therapy, equalization of R-R intervals suggests development of complete AV block due to Digoxin intoxication.
Rarely, complete AV block may be congenital.
References (some with links to free full text and sample ECGs)
Surawicz, Knilans. Chou's electrocardiography in clinical practice. 6th edition. Saunders. Philadelphia 2008.
Circulation 1995;92(3):442-449.
Br Med J (Clin Res Ed) 1983;286(6380):1769-1770.
Circulation 1995;92(3):283-285.
Br Heart J 1989;62(4):320-324.
G Ital Cardiol 1993;23(1):39-53.
Br Heart J 1990;64(5):338-339.
Clin Cardiol 1984;7(6):356-362.
Am J Cardiol 1991;67(4):225-230.
J Postgrad Med 1991;37(1):58B, 59-61.
J Clin Invest 1989;84(2):627-634.
Br Heart J 1988;60(6):512-515.
ECG 1. Third degree (complete) AV block in a 68 years-old woman with Systemic Sclerosis (Scleroderma).
Multidetector CT coronary angiography showed normal coronary arteries.
Click here for a more detailed ECG
The ECG above has been used with the permission of Anatolian Journal of Cardiology and AVES Publishing.
Click here to see the related article of Dr. Canpolat et al.
ECG 2. Third degree (complete) AV block. P waves are completely unrelated to the QRS complexes.
Click here for a more detailed ECG
ECG 3. The rhythm strip at the bottom of the above tracing shows complete AV block on the left ( P waves are not related to
QRS complexes ) which is then followed by 2:1 AV block ( only 1 of every two P waves is conducted ).
Click here for a more detailed ECG
ECG 4. The left side of above ECG shows complete AV block. P waves are not related to QRS complexes.
Some P waves, buried in the QRS, deform the QRS complex and give the impression of intermittent WPW syndrome at first glance
The right side shows Wenkebach AV block.
PR interval gradually prolongs; 3rd and 6th P waves are dropped (not conducted to the ventricles).
Click here for a more detailed ECG
ECG 5. The ECG above belongs to a 58 years-old man who admitted lately to the hospital and was diagnosed as
inferior myocardial infarction.
Q waves , ST segment elevation and negative T waves are seen in inferior leads.
Also, the P waves are not related to the QRS complexes : complete AV block .
Click here for a more detailed ECG
ECG 6. The ECG above belongs to a 55 years-old woman who developed persistent av block (A) after consumption of
Grayanotoxin-containing mad honey. The ECG on the right (B) was recorded after implantation of a permanent pacemaker.
Coronary angiography showed normal coronary arteries.
Click here for a more detailed ECG
The ECG above has been used with the permission of Anatolian Journal of Cardiology and AVES Publishing.
Click here to read the relevant article of Dr. Canpolat et al.
ECG 7. Complete AV block during acute myocardial infarction.
P waves are not related to QRS complexes.
Click here for a more detailed ECG
ECG 8. The ECG above shows complete AV block. P waves are not related to the QRS complexes,
At times, P waves are seen in front or at the end of the QRS complexes and distort them.
Pediatric cardiologist Prof. Dr. Birgul Varan has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 9a. The ECG above is from a 6 months-old baby with congenital complete AV block.
P waves are not related to the QRS complexes. Therefore, some P waves are buried in the QRS complexes.
P wave rate is normal for a baby; not to be confused with atrial flutter or atrial tachycardia.
Pediatric cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 9b. Rhythm tracing from the same baby: complete AV block is seen. P waves are not related to the QRS complexes.
P wave rate is normal for a baby; not to be confused with atrial flutter or atrial tachycardia.
Pediatric cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 10a. The above ECG shows both complete AV block and interatrial block. It was recorded during acute inferior wall myocardial infarction. P waves are not related to the QRS complexes. Therefore, some P waves are buried in QRS complexes. The P wave width is slightly more than 120 milliseconds: interatrial block. This ECG was recorded at a calibration of 20 mm/mV to show interatrial block. The P wave morphology and PR interval are also compatible with atrial infarction. Displacement of the PQ interval is considered the most useful sign of atrial infarction. The displacement of PQ interval during atrial infarction is best appreciated in patients with AV block.
Click here for a more detailed ECG
A close-up view of PR segment elevation from the ECG 10a is seen above. This is a magnified view of the P wave before the 8th QRS complex in lead II from the ECG 10a. The PR segment is elevated when compared with the baseline (TP segment).
ECG 10b. Above is his ECG at a standard 10 mm/mV calibration.
It is difficult to see interatrial block, PR segment elevation and complete AV block, at first glance.
Click here for a more detailed ECG
ECG 11a. The ECG above is from a 95 years-old woman with atrial fibrillation and complete av block.
Although atrial fibrillation is known as an "irregularly irregular rhythm", it becomes a regular rhythm
when complete av block developes. RR intervals are regular in the above ECG.
The above ECG is recorded at a standard calibration of 10mm/mV and the fibrillatory waves are hardly noticeable.
Click here for a more detailed ECG
ECG 11b. The above ECG belongs to the same patient.
It is recorded at a calibration of 20 mm/mV.
Now, it is more easy to see the fibrillatory waves.
The RR intervals are equal (regular) due to complete AV block.
Click here for a more detailed ECG
ECG 12a. Above is an ECG from a 44 years-old woman who had undergone catheter ablation of
supraventricular tachycardia 2 weeks ago. Complete AV block has developed during ablation.
Complete AV block is seen in the above ECG. Some QRS complexes are narrow (nodal beats) some are wide (ventricular beats).
The complete AV block is intermittent. To the right of the above ECG, the block disappears and
every P wave is followed by a QRS complex
Click here for a more detailed ECG
ECG 12b. The ECG above belongs to the same patient. It was recorded immediately after the ECG 12a.
Now, there is no complete AV block. The rhythm is sinus with right bundle branch block.
Click here for a more detailed ECG
ECG 13. The ECG above shows complete AV block. P waves are not related to the QRS complexes,
There is also right bundle branch block.
It was recorded 5 days after Bentall operation.
Click here for a more detailed ECG