d o t o r e g . c o m
t o r e g . c o m
Dr. Mete ALPASLAN
Torsades de Pointes- TdP
Diagnostic criteria
 TdP is a type of polymorphic ventricular tachycardia (VT) developing in patients with acquired or congenital long QT interval.
TdP is a type of polymorphic ventricular tachycardia (VT) developing in patients with acquired or congenital long QT interval.
If QT interval prolongation is lacking, then polymorphic VT is not accepted as TdP.
In the polymorphic VT of TdP, the QRS axis changes smoothly after a few complexes.
If TdP is detected during multichannel recording (Holter recording, etc.), some leads may show the typical polymorphic VT appearance while others may show monomorphic VT.
TdP usually has a rate of 200-250/minute but may also be 150-300/minute.
TdP is usually a self-terminating arrhythmia. Less frequently, it may degenerate into ventricular fibrillation.
Factors that favor the development of TdP
QT interval prolongation
Hypokalemia, less frequently hypomagnesemia or hypocalcemia
Certain drugs
Bradycardia, 2nd or 3rd degree AV block
Intracranial hemorrhage
Organophosphorus poisoning
Female gender
Links to similar ECGs
Open Cardiovasc Med J 2011; 5: 1-3.

ECG 1. Holter recording above shows development of Torsades de Pointes (TdP) due to bradycardia.
The ECG above, has been donated by Dr. Peter Kukla.
Click here for a more detailed ECG

ECG 2. Complete AV block resulting in the development of Torsades de Pointes (TdP).
The ECG above, has been donated by Dr. Peter Kukla.
Click here for a more detailed ECG

ECG 3. The ECG above, shows TdP which occurred after QT interval prolongation due to sotalol use in a 78 years old female.
The ECG above, has been donated by Dr. Peter Kukla.
Click here for a more detailed ECG

ECG 4. Short coupled Torsades de Pointes (TdP).
The above ECG has been donated by Dr. Antoine Leenhardt to our website.
Click here for a more detailed ECG

ECG 5. The ECG above is from a 77 years-old man with ischemic cardiomyopathy and was recorded during acute myocardial
infarction. Torsades de Pointes (TdP) is seen.
Click here for a more detailed ECG
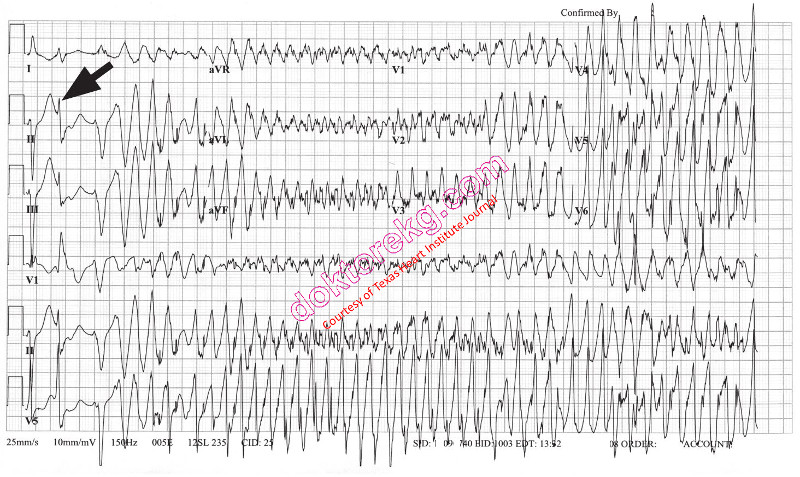
ECG 6a. The ECG above belongs to a 91 years-old woman who is at her scond day of levofloxacin therapy.
Torsades de Pointes (TdP) is seen.
The ECG above has been used with the permission of Texas Heart Institute Journal.
Click here for a more detailed ECG
Click here to go to the relevant article of the Texas Heart Institute Journal

ECG 6b. Above is her ECG repeated one minute later.
The TdP attack has terminated spontaneously and now the rhythm is sinus.
Leads aVL, V1 and V2 show Q waves while leads aVL and V1 to V4 show ST segment elevation.
Frequent VPCs and prolonged QT interval are also seen.
Acute coronary syndrome was suspected at first.
However, emergent coronary artery angiography revealed only minimal luminal irregularities.
Her cardiac enzymes were not elevated.
The ECG above has been used with the permission of Texas Heart Institute Journal.
Click here for a more detailed ECG
Click here to go to the relevant article of the Texas Heart Institute Journal
TdP is a type of polymorphic ventricular tachycardia (VT) developing in patients with acquired or congenital long QT interval.
If QT interval prolongation is lacking, then polymorphic VT is not accepted as TdP.
In the polymorphic VT of TdP, the QRS axis changes smoothly after a few complexes.
If TdP is detected during multichannel recording (Holter recording, etc.), some leads may show the typical polymorphic VT appearance while others may show monomorphic VT.
TdP usually has a rate of 200-250/minute but may also be 150-300/minute.
TdP is usually a self-terminating arrhythmia. Less frequently, it may degenerate into ventricular fibrillation.
Factors that favor the development of TdP
QT interval prolongation
Hypokalemia, less frequently hypomagnesemia or hypocalcemia
Certain drugs
Bradycardia, 2nd or 3rd degree AV block
Intracranial hemorrhage
Organophosphorus poisoning
Female gender
Links to similar ECGs
Open Cardiovasc Med J 2011; 5: 1-3.
ECG 1. Holter recording above shows development of Torsades de Pointes (TdP) due to bradycardia.
The ECG above, has been donated by Dr. Peter Kukla.
Click here for a more detailed ECG
ECG 2. Complete AV block resulting in the development of Torsades de Pointes (TdP).
The ECG above, has been donated by Dr. Peter Kukla.
Click here for a more detailed ECG
ECG 3. The ECG above, shows TdP which occurred after QT interval prolongation due to sotalol use in a 78 years old female.
The ECG above, has been donated by Dr. Peter Kukla.
Click here for a more detailed ECG
ECG 4. Short coupled Torsades de Pointes (TdP).
The above ECG has been donated by Dr. Antoine Leenhardt to our website.
Click here for a more detailed ECG
ECG 5. The ECG above is from a 77 years-old man with ischemic cardiomyopathy and was recorded during acute myocardial
infarction. Torsades de Pointes (TdP) is seen.
Click here for a more detailed ECG
ECG 6a. The ECG above belongs to a 91 years-old woman who is at her scond day of levofloxacin therapy.
Torsades de Pointes (TdP) is seen.
The ECG above has been used with the permission of Texas Heart Institute Journal.
Click here for a more detailed ECG
Click here to go to the relevant article of the Texas Heart Institute Journal
ECG 6b. Above is her ECG repeated one minute later.
The TdP attack has terminated spontaneously and now the rhythm is sinus.
Leads aVL, V1 and V2 show Q waves while leads aVL and V1 to V4 show ST segment elevation.
Frequent VPCs and prolonged QT interval are also seen.
Acute coronary syndrome was suspected at first.
However, emergent coronary artery angiography revealed only minimal luminal irregularities.
Her cardiac enzymes were not elevated.
The ECG above has been used with the permission of Texas Heart Institute Journal.
Click here for a more detailed ECG
Click here to go to the relevant article of the Texas Heart Institute Journal