doktorekg.com
Sinus Tachycardia
Diagnostic criteria
 Heart rate > 100/minute.
Heart rate > 100/minute.
P wave is positive in D1 and D2.
Every P wave is followed by a QRS complex.
About heart rate
Heart rate increases from birth to the end of the 1st month; then it starts to decrease again.
Since they have a high resting heart rate, sinus arrhythmia is rarely seen in NEWBORNs.
Sinus arrhythmia is more common in children and adolescents.
In the awake state, the normal range of heart rate in children is
91-166 /minute in the first week of NEWBORNs.
107-180 /minute at the end of the first month.
89-151 /minute at the end of the first year.
In an agitated or crying newborn, the heart rate may increase up to 220/minute.
A heart rate above 220/minute is always abnormal.
Causes of sinus tachycardia
Hypoxia
Hypovolemia
Anemia
Infection
Fever
Anxiety
Decompensated heart failure
Clinical significance of sinus tachycardia
Usually, there is an underlying cause of the sinus tachycardia.
Treatment of the underlying cause is usually sufficient for the disappearance of the sinus tachycardia.
Very rarely, there is no obvious cause for sinus tachycardia:
Inappropriate sinus tachycardia
.
If the patient complains of palpitation and the diagnosis is inappropriate
sinus tachycardia,
then heart rate can be decreased by the use of a beta blocker, diltiazem or verapamil.
Such a therapy may also prevent the possible development of tachycardia-induced cardiomyopathy.
Caution
If you cannot see P waves, do not diagnose sinus tachycardia.
If there is a regular tachycardia with narrow QRS complexes, the heart rate (ventricular rate) is
about 110-130/minute and P waves are not easily noticeable, then check for the presence of
atrial flutter with 2:1 block.
In such a case, look for evidence of "sawtooth appearance" in descending half of T waves.
In such a case, intravenous Adenosine administration may be helpful. Adenosine will result in a
transient increase in atrioventricular (AV) block and may reveal the presence of flutter waves.
If there is a regular tachycardia with narrow QRS complexes, the heart rate (ventricular rate) is
about 110-130/minute and P waves are not easily noticeable, then check for the presence of
ectopic atrial tachycardia with block.
In such a case, do NOT expect to see "sawtooth appearance".
In such a case, intravenous Adenosine administration may be helpful. Adenosine will result in a
transient increase in atrioventricular (AV) block and may reveal the presence of ectopic P waves.

ECG 1. Sinus tachycardia is seen above. P wave rate (atrial rate) is about 120/minute.

ECG 2. The above ECG belongs to a 22 years-old man who had received chemotherapy for AML.
ECHOcardiography showed dilated left ventricle and left atrium with depressed left ventricular systolic function
(low Ejection Fraction).
The rhythm is sinus tachycardia with a heart rate of 136/minute.
P waves and an acceptable PR interval are seen.
Click here for a more detailed ECG

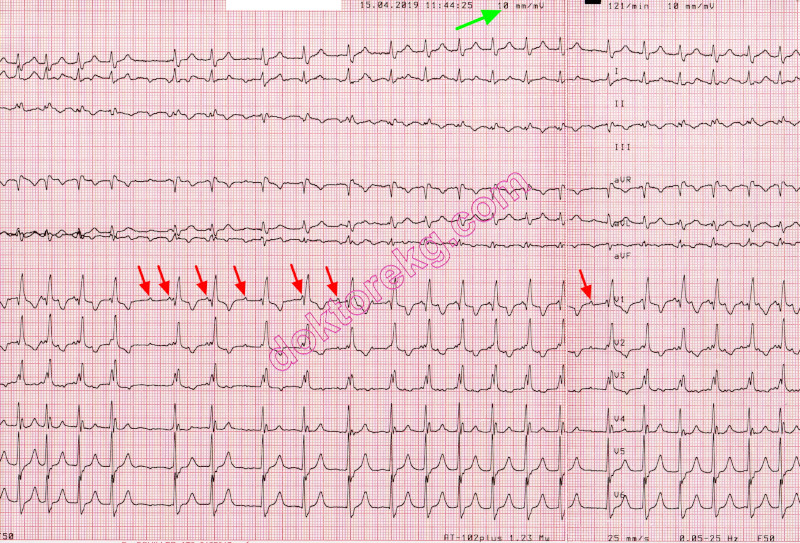
ECG 3a. The ECG above belongs to a 68 years-old man with Chronic Obstructive Pulmonary Disease (COPD).
He complains of dyspnea which worsened, recently.
His ECHOcardiogram showed normal left ventricular systolic function (normal Ejection Fraction).
The narrow QRS rhythm above has a heart rate of 123/minute.
Is it sinus tachycardia? Do we see P waves in lead V1?
The deflections in lead V1 cannot be P waves since they do not have an acceptable PR interval.
This ECG was recorded just before intravenous injection of 10 mg Adenosine.
The recording time is 10:09:39.
Click here for a more detailed ECG

ECG 3b. The above ECG belongs to the same patient and shows the onset of Adenosine effect.
It was recorded at 10:10:38 and shows the rhythm one minute after the ECG 3a.
Adenosine injection results in atrioventricular (AV) block and heart rate (ventricular rate) slows down.
When heart rate (ventricular rate) slows down, flutter waves become clearly visible.
This is atrial flutter. The rhythm in ECG 3a was atrial flutter.
When you see a regular narrow QRS tachycardia with a heart rate (ventricular rate, QRS rate) of 110-130/minute
but with no clearly identifiable P waves, remember the possibility of atrial flutter.
Click here for a more detailed ECG

ECG 3c. The above ECG belongs to the same patient and shows disappearance of Adenosine effect.
It was recorded at 10:10:49 (10 seconds after the ECG 3b).
With the disappearance of Adenosine effect, heart rate (ventricular rate) increases again.
With the disappearance of Adenosine effect, flutter waves become difficult to notice.
Click here for a more detailed ECG

ECG 4. The ECG above belongs to a 37 years-old man with overt anxiety.
Heart rate (ventricular rate) is 132/minute.
No sawtooth appearance is seen. The rhythm is sinus tachycardia.
P waves and (acceptable) PR interval are clearly seen.
On the other hand, the ECG 3a did not show clear P waves even though the heart rate was 123/minute.
Click here for a more detailed ECG

ECG 5. The ECG above belongs to a 79 years-old man with chronic obstructive pulmonary disease (COPD).
His heart rate (ventricular rate) is 122/minute.
Now, what do you think about the rhythm in the above ECG?
Do you see clear P waves and (an acceptable) PR interval?
Do you see sawtooth appearance (or at least some evidence of it)?
:))
It's clear, isn't it?
Click here for a more detailed ECG

ECG 6. The ECG above is from a 35 years-old man with atypical resting chest pain.
Heart rate (ventricular rate) is 122/minute.
P waves and (acceptable) PR interval are clearly seen.
Sawtooth appearance is not seen.
The rhythm is sinus tachycardia.
Many leads show PR depression while lead aVR shows PR elevation.
The clinical and ECG findings of this patient suggested the diagnosis of pericarditis.
Click here for a more detailed ECG

ECG 7. The ECG above is from a 47 years-old man.
Heart rate (ventricular rate) is 148/minute.
P waves and PR interval are clearly seen.
Even though the heart rate is high (148/minute), P waves are still seen.
Sawtooth appearance is not seen.
The rhythm is sinus tachycardia.
Click here for a more detailed ECG

ECG 8. The ECG above is from a 27 years-old man with chronic renal failure.
It was recorded a few hours after renal transplantation.
At the same time, his serum potassium level was measured as 5.1 mEq/L.
The rhythm is sinus tachycardia. The T waves and the P waves are clearly visible.
Click here for a more detailed ECG

ECG 9a. The ECG above belongs to a 85 years-old woman with coronary artery disease.
She complains of palpitation. Right bundle branch block is seen.
The heart rate is 121/minute. What is the rhythm?
Is it sinus tachycardia? Can you see the P waves?
Do you think that the PR interval is normal? Is it sinus tachycardia?
At a ventricular rate of 121/minute, it is easy to misdiagnose this rhyhtm as sinus tachycardia, at first glance.
Click here for a more detailed ECG

ECG 9b. The ECG above belongs to the same woman.
It was recorded 30 seconds after the ECG 9a.
What is the rhythm?
Do you see the P waves? Do you think that the PR interval is normal?
Do you think that there is sawtooth appearance?
Click here for a more detailed ECG

ECG 9c. The above rhythm tracing belongs to the same woman.
It was recorded at a calibration of 20 mm/mV to better see the details.
P waves are clearly seen. Atrial rate (P wave rate) is 240/minute.
Not all P waves are conducted to ventricles. This is ectopic atrial tachycardia with block.
This is not atrial flutter, there is no sawtooth appearance: a flat baseline between the P waves is seen.
Since frequent temporary increases in AV block level revealed ectopic P waves, we did not need to use Adenosine
in this patient.
Click here for a more detailed ECG
ECG 9d. The above rhythm tracing belongs to the same woman.
It was recorded at a calibration of 10 mm/mV
P waves are seen. Not all P waves are conducted to the ventricles.
This is ectopic atrial tachycardia with block.
Since frequent temporary increases in AV block level revealed ectopic P waves, we did not need to use Adenosine
in this patient.
Click here for a more detailed ECG

ECG 10a. The ECG above belongs to a 66 years-old woman with coronary artery disease and mitral valve prosthesis.
She had undergone coronary artery bypass grafting operation and mitral valve replacement 2 weeks ago.
She had experienced inferoposterior wall myocardial infarction before the operation.
Now she has left ventricular systolic dysfunction with Ejection Fraction (EF) of 35%.
She is under Bisoprolol (beta blocker) therapy.
Her heart rate is 110/minute.
What is the rhythm? Is it sinus tachycardia?
Click here for a more detailed ECG

ECG 10b. The ECG above belongs to the same woman. It was recorded 3 weeks after the ECG 10a.
This ECG was recorded at a standard calibration of 10 mm/mV and at a paper speed of 25 mm/second.
After 3 weeks, her heart rate is almost the same: 111/minute.
She is still taking Bisoprolol (beta blocker).
What is the rhythm? Is it sinus tachycardia?
Do you see P waves? Is there a normal PR interval?
Click here for a more detailed ECG

ECG 10c. The ECG above belongs to the same woman. It was recorded immediately after the ECG 10b.
To see the details clearly, the calibration was now set at 20 mm/mV.
Her heart rate is 110/minute.
Seemingly P waves in lead V1 are in fact flutter waves.
Flutter waves deform terminal portion of the QRS complexes in inferior leads.
The rhythm is atrial flutter, not sinus tachycardia.
Click here for a more detailed ECG

ECG 10d. The ECG above belongs to the same woman. It was recorded 36 days after the ECG 10c.
This time, the rhythm is sinus tachycardia with a heart rate of 104/minute.
Leads II and V1 clearly show P waves with normal PR interval.
Click here for a more detailed ECG

ECG 11a. The ECG above belongs to a 70 years-old hypertensive woman with coronary artery disease.
She complains of palpitation.
The above ECG was recorded in another hospital and the patient was referred to our clinic.
It was recorded at a standard calibration of 10 mm/mV and at a standard paper speed of 25 mm/sec.
Click here for a more detailed ECG

ECG 11b. The ECG above belongs to the same woman.
It was recorded in our clinic, on the same day with the ECG 11a.
Its calibration is 10 mm/mV at a paper speed of 25 mm/sec (standard settings).
Do you see P waves? Is this rhythm sinus tachycardia?
Click here for a more detailed ECG

ECG 11c. The 6-channel rhythm tracing above belongs to the same woman.
It was recorded in our clinic immediately after the ECG 11b.
To see flutter waves clearly, the paper speed was set at 50 mm/second.
The rhythm is atrial flutter, not sinus tachycardia.
Click here for a more detailed ECG

ECG 11d. The 6-channel rhythm tracing above belongs to the same woman.
It was recorded immediately after the ECG 11c.
It was recorded at a calibration of 20 mm/mV and a paper speed of 50 mm/second.
Now flutter waves are seen clearly.
The rhythm is atrial flutter, not sinus tachycardia.
Click here for a more detailed ECG
Diagnostic criteria
Heart rate > 100/minute.
P wave is positive in D1 and D2.
Every P wave is followed by a QRS complex.
About heart rate
Heart rate increases from birth to the end of the 1st month; then it starts to decrease again.
Since they have a high resting heart rate, sinus arrhythmia is rarely seen in NEWBORNs.
Sinus arrhythmia is more common in children and adolescents.
In the awake state, the normal range of heart rate in children is
91-166 /minute in the first week of NEWBORNs.
107-180 /minute at the end of the first month.
89-151 /minute at the end of the first year.
In an agitated or crying newborn, the heart rate may increase up to 220/minute.
A heart rate above 220/minute is always abnormal.
Causes of sinus tachycardia
Hypoxia
Hypovolemia
Anemia
Infection
Fever
Anxiety
Decompensated heart failure
Clinical significance of sinus tachycardia
Usually, there is an underlying cause of the sinus tachycardia.
Treatment of the underlying cause is usually sufficient for the disappearance of the sinus tachycardia.
Very rarely, there is no obvious cause for sinus tachycardia:
Inappropriate sinus tachycardia
.
If the patient complains of palpitation and the diagnosis is inappropriate
sinus tachycardia, then heart rate can be decreased by the use of a beta blocker, diltiazem or verapamil.
Such a therapy may also prevent the possible development of tachycardia-induced cardiomyopathy.
Caution
If you cannot see P waves, do not diagnose sinus tachycardia.
If there is a regular tachycardia with narrow QRS complexes, the heart rate (ventricular rate) is
about 110-130/minute and P waves are not easily noticeable, then check for the presence of
atrial flutter with 2:1 block.
In such a case, look for evidence of "sawtooth appearance" in descending half of T waves.
In such a case, intravenous Adenosine administration may be helpful. Adenosine will result in a
transient increase in atrioventricular (AV) block and may reveal the presence of flutter waves.
If there is a regular tachycardia with narrow QRS complexes, the heart rate (ventricular rate) is
about 110-130/minute and P waves are not easily noticeable, then check for the presence of
ectopic atrial tachycardia with block.
In such a case, do NOT expect to see "sawtooth appearance".
In such a case, intravenous Adenosine administration may be helpful. Adenosine will result in a
transient increase in atrioventricular (AV) block and may reveal the presence of ectopic P waves.
ECG 1. Sinus tachycardia is seen above. P wave rate (atrial rate) is about 120/minute.
ECG 2. The above ECG belongs to a 22 years-old man who had received chemotherapy for AML.
ECHOcardiography showed dilated left ventricle and left atrium with depressed left ventricular systolic function
(low Ejection Fraction).
The rhythm is sinus tachycardia with a heart rate of 136/minute.
P waves and an acceptable PR interval are seen.
Click here for a more detailed ECG
ECG 3a. The ECG above belongs to a 68 years-old man with Chronic Obstructive Pulmonary Disease (COPD).
He complains of dyspnea which worsened, recently.
His ECHOcardiogram showed normal left ventricular systolic function (normal Ejection Fraction).
The narrow QRS rhythm above has a heart rate of 123/minute.
Is it sinus tachycardia? Do we see P waves in lead V1?
The deflections in lead V1 cannot be P waves since they do not have an acceptable PR interval.
This ECG was recorded just before intravenous injection of 10 mg Adenosine.
The recording time is 10:09:39.
Click here for a more detailed ECG
ECG 3b. The above ECG belongs to the same patient and shows the onset of Adenosine effect.
It was recorded at 10:10:38 and shows the rhythm one minute after the ECG 3a.
Adenosine injection results in atrioventricular (AV) block and heart rate (ventricular rate) slows down.
When heart rate (ventricular rate) slows down, flutter waves become clearly visible.
This is atrial flutter. The rhythm in ECG 3a was atrial flutter.
When you see a regular narrow QRS tachycardia with a heart rate (ventricular rate, QRS rate) of 110-130/minute
but with no clearly identifiable P waves, remember the possibility of atrial flutter.
Click here for a more detailed ECG
ECG 3c. The above ECG belongs to the same patient and shows disappearance of Adenosine effect.
It was recorded at 10:10:49 (10 seconds after the ECG 3b).
With the disappearance of Adenosine effect, heart rate (ventricular rate) increases again.
With the disappearance of Adenosine effect, flutter waves become difficult to notice.
Click here for a more detailed ECG
ECG 4. The ECG above belongs to a 37 years-old man with overt anxiety.
Heart rate (ventricular rate) is 132/minute.
No sawtooth appearance is seen. The rhythm is sinus tachycardia.
P waves and (acceptable) PR interval are clearly seen.
On the other hand, the ECG 3a did not show clear P waves even though the heart rate was 123/minute.
Click here for a more detailed ECG
ECG 5. The ECG above belongs to a 79 years-old man with chronic obstructive pulmonary disease (COPD).
His heart rate (ventricular rate) is 122/minute.
Now, what do you think about the rhythm in the above ECG?
Do you see clear P waves and (an acceptable) PR interval?
Do you see sawtooth appearance (or at least some evidence of it)?
:))
It's clear, isn't it?
Click here for a more detailed ECG
ECG 6. The ECG above is from a 35 years-old man with atypical resting chest pain.
Heart rate (ventricular rate) is 122/minute.
P waves and (acceptable) PR interval are clearly seen.
Sawtooth appearance is not seen.
The rhythm is sinus tachycardia.
Many leads show PR depression while lead aVR shows PR elevation.
The clinical and ECG findings of this patient suggested the diagnosis of pericarditis.
Click here for a more detailed ECG
ECG 7. The ECG above is from a 47 years-old man.
Heart rate (ventricular rate) is 148/minute.
P waves and PR interval are clearly seen.
Even though the heart rate is high (148/minute), P waves are still seen.
Sawtooth appearance is not seen.
The rhythm is sinus tachycardia.
Click here for a more detailed ECG
ECG 8. The ECG above is from a 27 years-old man with chronic renal failure.
It was recorded a few hours after renal transplantation.
At the same time, his serum potassium level was measured as 5.1 mEq/L.
The rhythm is sinus tachycardia. The T waves and the P waves are clearly visible.
Click here for a more detailed ECG
ECG 9a. The ECG above belongs to a 85 years-old woman with coronary artery disease.
She complains of palpitation. Right bundle branch block is seen.
The heart rate is 121/minute. What is the rhythm?
Is it sinus tachycardia? Can you see the P waves?
Do you think that the PR interval is normal? Is it sinus tachycardia?
At a ventricular rate of 121/minute, it is easy to misdiagnose this rhyhtm as sinus tachycardia, at first glance.
Click here for a more detailed ECG
ECG 9b. The ECG above belongs to the same woman.
It was recorded 30 seconds after the ECG 9a.
What is the rhythm?
Do you see the P waves? Do you think that the PR interval is normal?
Do you think that there is sawtooth appearance?
Click here for a more detailed ECG
ECG 9c. The above rhythm tracing belongs to the same woman.
It was recorded at a calibration of 20 mm/mV to better see the details.
P waves are clearly seen. Atrial rate (P wave rate) is 240/minute.
Not all P waves are conducted to ventricles. This is ectopic atrial tachycardia with block.
This is not atrial flutter, there is no sawtooth appearance: a flat baseline between the P waves is seen.
Since frequent temporary increases in AV block level revealed ectopic P waves, we did not need to use Adenosine
in this patient.
Click here for a more detailed ECG
ECG 9d. The above rhythm tracing belongs to the same woman.
It was recorded at a calibration of 10 mm/mV
P waves are seen. Not all P waves are conducted to the ventricles.
This is ectopic atrial tachycardia with block.
Since frequent temporary increases in AV block level revealed ectopic P waves, we did not need to use Adenosine
in this patient.
Click here for a more detailed ECG
ECG 10a. The ECG above belongs to a 66 years-old woman with coronary artery disease and mitral valve prosthesis.
She had undergone coronary artery bypass grafting operation and mitral valve replacement 2 weeks ago.
She had experienced inferoposterior wall myocardial infarction before the operation.
Now she has left ventricular systolic dysfunction with Ejection Fraction (EF) of 35%.
She is under Bisoprolol (beta blocker) therapy.
Her heart rate is 110/minute.
What is the rhythm? Is it sinus tachycardia?
Click here for a more detailed ECG
ECG 10b. The ECG above belongs to the same woman. It was recorded 3 weeks after the ECG 10a.
This ECG was recorded at a standard calibration of 10 mm/mV and at a paper speed of 25 mm/second.
After 3 weeks, her heart rate is almost the same: 111/minute.
She is still taking Bisoprolol (beta blocker).
What is the rhythm? Is it sinus tachycardia?
Do you see P waves? Is there a normal PR interval?
Click here for a more detailed ECG
ECG 10c. The ECG above belongs to the same woman. It was recorded immediately after the ECG 10b.
To see the details clearly, the calibration was now set at 20 mm/mV.
Her heart rate is 110/minute.
Seemingly P waves in lead V1 are in fact flutter waves.
Flutter waves deform terminal portion of the QRS complexes in inferior leads.
The rhythm is atrial flutter, not sinus tachycardia.
Click here for a more detailed ECG
ECG 10d. The ECG above belongs to the same woman. It was recorded 36 days after the ECG 10c.
This time, the rhythm is sinus tachycardia with a heart rate of 104/minute.
Leads II and V1 clearly show P waves with normal PR interval.
Click here for a more detailed ECG
ECG 11a. The ECG above belongs to a 70 years-old hypertensive woman with coronary artery disease.
She complains of palpitation.
The above ECG was recorded in another hospital and the patient was referred to our clinic.
It was recorded at a standard calibration of 10 mm/mV and at a standard paper speed of 25 mm/sec.
Click here for a more detailed ECG
ECG 11b. The ECG above belongs to the same woman.
It was recorded in our clinic, on the same day with the ECG 11a.
Its calibration is 10 mm/mV at a paper speed of 25 mm/sec (standard settings).
Do you see P waves? Is this rhythm sinus tachycardia?
Click here for a more detailed ECG
ECG 11c. The 6-channel rhythm tracing above belongs to the same woman.
It was recorded in our clinic immediately after the ECG 11b.
To see flutter waves clearly, the paper speed was set at 50 mm/second.
The rhythm is atrial flutter, not sinus tachycardia.
Click here for a more detailed ECG
ECG 11d. The 6-channel rhythm tracing above belongs to the same woman.
It was recorded immediately after the ECG 11c.
It was recorded at a calibration of 20 mm/mV and a paper speed of 50 mm/second.
Now flutter waves are seen clearly.
The rhythm is atrial flutter, not sinus tachycardia.
Click here for a more detailed ECG