doktorekg.com
Atrioventricular Nodal Reciprocating Tachycardia - AVNRT
Diagnostic criteria
 Heart rate (ventricular rate) is 140-250/minute.
Heart rate (ventricular rate) is 140-250/minute.
QRS complexes are narrow (<120ms) and are similar to those of the sinus rhythm.
This is the most common type of paroxsymal supraventricular tachycardias.
Although not a criteria in the differential diagnosis, the ventricular rate in supraventricular tachycardias is generally higher than the ventricular rate of the ventricular tachycardias.
Clinical importance
In patients with narrow QRS complex, paroxysmal, re-entrant supraventricular tachycardias, the appearance of ST segment depression or T wave negativity during tachycardia does not signify the presence of coronary artery disease.
In patients with narrow QRS complex, paroxysmal, re-entrant supraventricular tachycardias, the appearance of new T wave negativity after tachycardia has ended, does not signify the presence of coronary artery disease.

ECG 1. AVNRT. Tachycardia with narrow QRS complexes.
Click here for a more detailed ECG

ECG 2.AVNRT in another patient.
Click here for a more detailed ECG
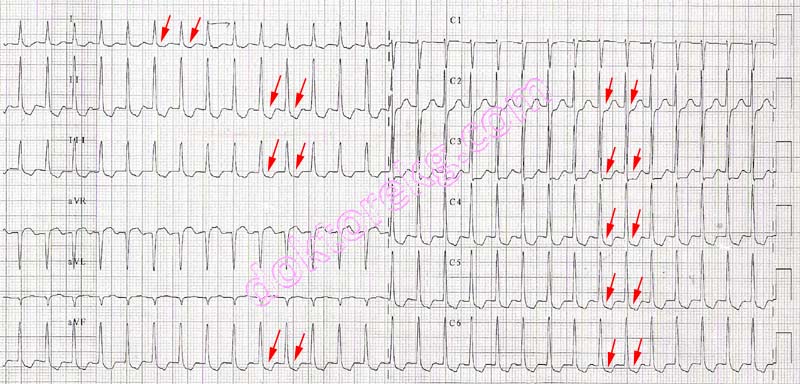
ECG 3a. Widespread ST segment depression is observed in a middle-aged woman with AVNRT.
Click here for a more detailed ECG

ECG 3b. In the same patient, ST segment depression disappeared immediately after the tachycardia has ended.
Click here for a more detailed ECG

ECG 4. A 5 years old child with dilated cardiomyopathy and long RP AVNRT. P waves preceeding the QRS complexes are
negative in leads II, III and aVF (positive in lead aVR) and are formed by the retrograde activation of the atrium. This patient
later underwent successful radiofrequency ablation. The calibration of ECG is 5 mm/mV.
Prof. Dr. Bulent Oran has donated this ECG to our website.
Click here for a more detailed ECG

ECG 5a. Supraventricular tachycardia (SVT) attack in a 1 day-old newborn.
Pediatric Cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 5b. The ECG above belongs to the same baby and shows SVT attack under Amiodarone therapy.
It was recorded when he was 5 days-old.
Pediatric Cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 6a. The ECG above is from a 69 years-old woman with the complaints of palpitation and dyspnoea.
The rhythm may seem like supraventricular tachycardia at first glance.
However, it is atrial fibrillation with a rapid ventricular response.
The rhythm is irregularly irregular.
Cardiologist Sinan Altan Kocaman has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 6b. The above ECG belongs to the same patient. It was recorded 20 hours after the ECG 27a.
Medical therapy slowed the ventricular response.
The rhythm is still atrial fibrillation: irregularly irregular with no P waves.
Cardiologist Sinan Altan Kocaman has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 7. The ECG above belongs to a 68 years-old woman with normal coronary arteries.
The rhythm seems like wide QRS complex tachycardia at first glance.
The ECG's computer also indicates "Wide QRS tachycardia, Nonspecific intraventricular block".
However, the computer's comment is wrong. If looked carefully, it will be noted that this is a narrow QRS tachycardia.
Just look at the interval between the onset of QRS complex and J point.
The patient underwent electrophysiological study (EPS) which showed atypical atrioventricular nodal reentrant
tachycardia (AVNRT). Successful ablation was performed.
Cardiologist Sinan Altan Kocaman has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 8a. The ECG above belongs to a 39 years-old man with palpitation.
The rhythm is narrow QRS tachycardia with a heart rate of 198/minute.
The patient underwent electrophysiological study (EPS) which showed atrioventricular nodal reentrant
tachycardia (AVNRT). Successful ablation was performed.
Click here for a more detailed ECG

ECG 8b. The ECG above belongs to the same man. It was recorded after termination of the supraventricular tachycardia,
but before catheter ablation.
Click here for a more detailed ECG

ECG 9a. The ECG above shows alternans of both QRS amplitude and RR intervals.
Prof. Dr. Hakan Gullu has donated the above ECG to our website.
Click here for a more detailed ECG

ECG 9b. The ECG above belongs to the same woman.
It was recorded 18 minutes after the ECG 9a.
Supraventricular tachycardia disappeared.
Both QRS amplitude alternans and RR interval alternans disappeared.
Prof. Dr. Hakan Gullu has donated the above ECG to our website.
Click here for a more detailed ECG
Diagnostic criteria
Heart rate (ventricular rate) is 140-250/minute.
QRS complexes are narrow (<120ms) and are similar to those of the sinus rhythm.
This is the most common type of paroxsymal supraventricular tachycardias.
Although not a criteria in the differential diagnosis, the ventricular rate in supraventricular tachycardias is generally higher than the ventricular rate of the ventricular tachycardias.
Clinical importance
In patients with narrow QRS complex, paroxysmal, re-entrant supraventricular tachycardias, the appearance of ST segment depression or T wave negativity during tachycardia does not signify the presence of coronary artery disease.
In patients with narrow QRS complex, paroxysmal, re-entrant supraventricular tachycardias, the appearance of new T wave negativity after tachycardia has ended, does not signify the presence of coronary artery disease.
ECG 1. AVNRT. Tachycardia with narrow QRS complexes.
Click here for a more detailed ECG
ECG 2.AVNRT in another patient.
Click here for a more detailed ECG
ECG 3a. Widespread ST segment depression is observed in a middle-aged woman with AVNRT.
Click here for a more detailed ECG
ECG 3b. In the same patient, ST segment depression disappeared immediately after the tachycardia has ended.
Click here for a more detailed ECG
ECG 4. A 5 years old child with dilated cardiomyopathy and long RP AVNRT. P waves preceeding the QRS complexes are
negative in leads II, III and aVF (positive in lead aVR) and are formed by the retrograde activation of the atrium. This patient
later underwent successful radiofrequency ablation. The calibration of ECG is 5 mm/mV.
Prof. Dr. Bulent Oran has donated this ECG to our website.
Click here for a more detailed ECG
ECG 5a. Supraventricular tachycardia (SVT) attack in a 1 day-old newborn.
Pediatric Cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 5b. The ECG above belongs to the same baby and shows SVT attack under Amiodarone therapy.
It was recorded when he was 5 days-old.
Pediatric Cardiologist Dr. Mahmut Gokdemir has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 6a. The ECG above is from a 69 years-old woman with the complaints of palpitation and dyspnoea.
The rhythm may seem like supraventricular tachycardia at first glance.
However, it is atrial fibrillation with a rapid ventricular response.
The rhythm is irregularly irregular.
Cardiologist Sinan Altan Kocaman has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 6b. The above ECG belongs to the same patient. It was recorded 20 hours after the ECG 27a.
Medical therapy slowed the ventricular response.
The rhythm is still atrial fibrillation: irregularly irregular with no P waves.
Cardiologist Sinan Altan Kocaman has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 7. The ECG above belongs to a 68 years-old woman with normal coronary arteries.
The rhythm seems like wide QRS complex tachycardia at first glance.
The ECG's computer also indicates "Wide QRS tachycardia, Nonspecific intraventricular block".
However, the computer's comment is wrong. If looked carefully, it will be noted that this is a narrow QRS tachycardia.
Just look at the interval between the onset of QRS complex and J point.
The patient underwent electrophysiological study (EPS) which showed atypical atrioventricular nodal reentrant
tachycardia (AVNRT). Successful ablation was performed.
Cardiologist Sinan Altan Kocaman has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 8a. The ECG above belongs to a 39 years-old man with palpitation.
The rhythm is narrow QRS tachycardia with a heart rate of 198/minute.
The patient underwent electrophysiological study (EPS) which showed atrioventricular nodal reentrant
tachycardia (AVNRT). Successful ablation was performed.
Click here for a more detailed ECG
ECG 8b. The ECG above belongs to the same man. It was recorded after termination of the supraventricular tachycardia,
but before catheter ablation.
Click here for a more detailed ECG
ECG 9a. The ECG above shows alternans of both QRS amplitude and RR intervals.
Prof. Dr. Hakan Gullu has donated the above ECG to our website.
Click here for a more detailed ECG
ECG 9b. The ECG above belongs to the same woman.
It was recorded 18 minutes after the ECG 9a.
Supraventricular tachycardia disappeared.
Both QRS amplitude alternans and RR interval alternans disappeared.
Prof. Dr. Hakan Gullu has donated the above ECG to our website.
Click here for a more detailed ECG